Our Mission
Welcome to CTE Matters to Me.
Our mission is to:
- raise awareness of CTE - chronic traumatic encephalopathy - especially in New Zealand
- raise awareness of the devastating and tragic consequences of misdiagnosing brain injury as a 'mental health' or 'psychiatric' issue
- raise awareness of the need for medical education & training which includes the identification of brain injury and suspected CTE
- collate links to information about treatment for people who have suspected CTE
- provide mutual support, understanding and networking among people and families of those who have suspected CTE
- present our hypothesis of 'The Pono and Tika Pattern' as distinct symptoms and markers of CTE, and invite feedback
- develop a standard of care for people who have suspected CTE.

Ange Murtha, at far right, in late 2011.
Shine a light on CTE
Update - We are thrilled to advise that we've reached our goal!
With immense gratitide to everyone who donated to Ange's Give-a-little page, and with special thanks to The Billy Guyton Foundation whose generous donation got Ange across the finish line. Ange will soon be able to purchase the Vielight and when it arrives she'll be able to start using it. We'll post updates here.
The work doesn't stop here though. If you would like to support others like Ange, please consider supporting the Give-a-Little page for The Billy Guyton Foundation.
The following will soon be archived:
Help Ange Heal — and Prove It's Possible for Others
Ange is an all-round sportswoman from Hokitika on the West Coast. Like so many Kiwis, she grew up living the active outdoor life — rugby, skiing, snowboarding, mountain biking. She'd completed a horticulture diploma and was building a new career when, in 2011, after years of repeated head knocks since childhood, she had her first seizure just eight days after her last rugby game of the season.
Instead of being treated for brain injury, Ange was misdiagnosed with a psychiatric condition. She was later forcibly detained in a psychiatric unit and drugged for something she does not have.
For fourteen years, Ange kept saying: "This is from the head knocks. I have a brain injury."
To this day, Ange has never received proper treatment for her brain injury. The last care she had was from a concussion team in 2016 — before the system shut her out.
But Ange hasn't given up.
Even while experiencing progressive decline, she has connected with the international CTE community and found purpose in helping others facing the same fight. Through 'CTE Matters To Me', Ange and Elisabeth are working to raise awareness, challenge the systems that failed her, and support others affected by brain injury.
Now Ange wants to heal — not a miracle cure, but real, tangible improvement. And she wants to prove it's possible for others too.
What is a Vielight?
The Vielight Neuro Gamma 4 is the world's most researched brain photobiomodulation device. It delivers near-infrared light through the skull and nasal passage to reach deep brain structures, stimulating mitochondria at a cellular level to help damaged brain cells heal. It's backed by over 35 published clinical trials across conditions including traumatic brain injury, Alzheimer's, and cognitive decline.
This isn't experimental wishful thinking — it's cutting-edge neuroscience, and it could be a game-changer for Ange.
How You Can Help
We're raising NZ$3,700 to cover the cost of the device, international shipping, customs duties, and platform fees.
Every dollar brings Ange closer to healing — and helps prove that hope is real for everyone living with brain injury.
As Ange says: "The only way through is together."
Update- We've made it!!! With huge thanks to everyone who donated. We'll post updates here.

This is a Vielight Neuro Gamma 4. This is what we are fundraising for to help give Ange some relief.
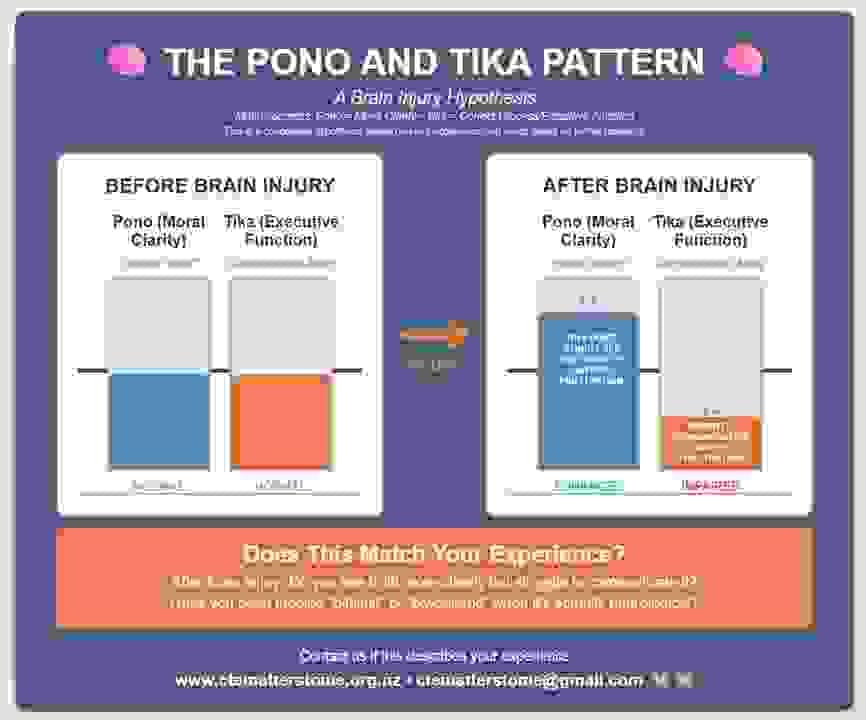
The Pono and Tika pattern
In our conversations about brain injury and CTE, Ange and I have noticed a common pattern, which is that people with brain injuries often experience two things at once:
1. enhanced moral clarity- i.e. seeing the truth and wondering why others can't see it too, which leads to intense frustration, and
2. impaired and inhibited communication, which also leads to intense frustration.
It seems to us that this combination of experiences leads to anger and grief (which is not the same as 'depression'). These issues are neurological, not psychological or 'psychiatric'.
Does this match your experience? If so, we'd love to hear from you.